Category Archives: Prepayment Review
Premature Recoupment of Medicare or Medicaid Funds Can Feel Like Getting Mauled by Dodgeballs: But Is It Constitutional?
State and federal governments contract with many private vendors to manage Medicare and Medicaid. And regulatory audits are fair game for all these contracted vendors and, even more – the government also contracts with private companies that are specifically hired to audit health care providers. Not even counting the contracted vendors that manage Medicaid or Medicare (the companies to which you bill and get paid), we have Recovery Act Contractors (RAC), Zone Program Integrity Contractors (ZPICs), Medicare Administrative Contractors (MACs), and Comprehensive Error Rate Testing (CERT) auditors. See blog for explanation. ZPICs, RACs, and MACs conduct pre-payment audits. ZPICs, RACs, MACs, and CERTs conduct post-payment audits.
It can seem that audits can hit you from every side.

“Remember the 5 D’s of dodgeball: Dodge, duck, dip, dive and dodge.”
Remember the 5 A’s of audits: Appeal, argue, apply, attest, and appeal.”
Medicare providers can contest payment denials (whether pre-payment or post-payment) through a five-level appeal process. See blog.
On the other hand, Medicaid provider appeals vary depending on which state law applies. For example, in NC, the general process is an informal reconsideration review (which has .008% because, essentially you are appealing to the very entity that decided you owed an overpayment), then you file a Petition for Contested Case at the Office of Administrative Hearings (OAH). Your likelihood of success greatly increases at the OAH level because these hearings are conducted by an impartial judge. Unlike in New Mexico, where the administrative law judges are hired by Human Services Department, which is the agency that decided you owe an overpayment. In NM, your chance of success increases greatly on judicial review.
In Tx, providers may use three methods to appeal Medicaid fee-for-service and carve-out service claims to Texas Medicaid & Healthcare Partnership (TMHP): electronic, Automated Inquiry System (AIS), or paper within 120 days.
In Il, you have 60-days to identify the total amount of all undisputed and disputed audit
overpayment. You must report, explain and repay any overpayment, pursuant to 42 U.S.C.A. Section 1320a-7k(d) and Illinois Public Aid Code 305 ILCS 5/12-4.25(L). The OIG will forward the appeal request pertaining to all disputed audit overpayments to the Office of Counsel to the Inspector General for resolution. The provider will have the opportunity to appeal the Final Audit Determination, pursuant to the hearing process established by 89 Illinois Adm. Code, Sections 104 and 140.1 et. seq.
You get the point.”Nobody makes me bleed my own blood. Nobody!” – White Goodman
Recoupment During Appeals
Regardless whether you are appealing a Medicare or Medicaid alleged overpayment, the appeals process takes time. Years in some circumstances. While the time gently passes during the appeal process, can the government or one of its minions recoup funds while your appeal is pending?
The answer is: It depends.
Before I explain, I hear my soapbox calling, so I will jump right on it. It is my legal opinion (and I am usually right) that recoupment prior to the appeal process is complete is a violation of due process. People are always shocked how many laws and regulations, both on the federal and state level, are unconstitutional. People think, well, that’s the law…it must be legal. Incorrect. Because something is allowed or not allowed by law does not mean the law is constitutional. If Congress passed a law that made it illegal to travel between states via car, that would be unconstitutional. In instances that the government is allowed to recoup Medicaid/care prior to the appeal is complete, in my (educated) opinion. However, until a provider will fund a lawsuit to strike these allowances, the rules are what they are. Soapbox – off.
Going back to whether recoupment may occur before your appeal is complete…
For Medicare audit appeals, there can be no recoupment at levels one and two. After level two, however, the dodgeballs can fly, according to the regulations. Remember, the time between levels two and three can be 3 – 5 years, maybe longer. See blog. There are legal options for a Medicare provider to stop recoupments during the 3rd through 5th levels of appeal and many are successful. But according to the black letter of the law, Medicare reimbursements can be recouped during the appeal process.
Medicaid recoupment prior to the appeal process varies depending on the state. Recoupment is not allowed in NC while the appeal process is ongoing. Even if you reside in a state that allows recoupment while the appeal process is ongoing – that does not mean that the recoupment is legal and constitutional. You do have legal rights! You do not need to be the last kid in the middle of a dodgeball game.
Don’t be this guy:

Inpatient Rehabilitation Facility Stay Claim Denials – Appeal Those Findings!
Centers for Medicare & Medicaid Services (CMS) created a new page on its Recovery Audit Contractor (RAC) website entitled “Provider Resources.” CMS indicated that it will post on this page any new issues the RACs have proposed to audit and are being evaluated by CMS for approval. It is like a glimpse behind the curtain to see the Great Oz. This is a fantastic resource for providers. CMS posts a list of review topics that have been proposed, but not yet approved, for RACs to review. You can see the future!
Topics proposed for future audits:
- Inpatient Rehabilitation Facility (IRF) Stays: Meeting Requirements to be considered Reasonable and Necessary;
- Respiratory Assistive Devices: Meeting Requirements to be considered Reasonable and Necessary;
- Excessive or Insufficient Drugs and Biologicals Units Billed;
- E&M Codes billed within a Procedure Code with a “0” Day Global Period (Endoscopies or some minor surgical procedures);
- E&M Codes billed within a Procedure Code with a “10” Day Global Period (other minor procedures);
- E&M Codes billed within a Procedure Code with a “90” Day Global Period (major surgeries);
Over the next few weeks, intermittently (along with other blog posts), I will tackle these, and other, hot RAC audit topics.
IRFs are under fire in North Carolina, South Carolina, Virginia, and West Virginia!
Many patients with conditions like stroke or brain injury, who need an intensive medical rehabilitation program, are transferred to an inpatient rehabilitation facility.
Palmetto, one of Medicare’s MACs, conducted a prepayment review of IRFs in these four states. The results were bleak, indeed, and will, most likely, spur more audits of IRFs in the future. If you are a Medicare provider within Palmetto’s catchment area, then you know that Palmetto conducts a lot of targeted prepayment review. Here is a map of the MAC jurisdictions:

You can see that Palmetto manages Medicare for North Carolina, South Carolina, West Virginia, and Virginia. So Palmetto’s prepayment review covered its entire catchment area.
North Carolina Results A total of 28 claims were reviewed with 19 of the claims either completely or partially denied. The total dollars reviewed was $593,174.60 of which $416,483.42 was denied, resulting in a charge denial rate of 70.2 percent.
South Carolina Results A total of 24 claims were reviewed with 16 of the claims either completely or partially denied. The total dollars reviewed was $484,742.68 of which $325,266.43 was denied, resulting in a charge denial rate of 67.1 percent.
West Virginia Results
A total of two claims were reviewed with two of the claims either completely or partially denied. The total dollars reviewed was $32,506.21 of which $32,506.21 was denied, resulting in a charge denial rate of 100 percent.
Virginia Results
A total of 39 claims were reviewed with 31 of the claims either completely or partially denied. The total dollars reviewed was $810,913.83 of which $629,118.08 was denied, resulting in a charge denial rate of 77.6 percent.
In all 4 states, the most cited denial code was “5J504,” which means that “need for service/item not medically and reasonably necessary.” Subjective, right? I mean, who is better at determining medical necessity: (1) the treating physician who actually performs services and conducts the physical; or (2) a utilization auditor without an MD and who as never rendered medical services on the particular consumer? I see it all the time…former dental hygienists review the medical records of dentists and determine that no medial necessity exists…
When it comes to IRF Stays, what is reasonable and necessary?
According to Medicare policy and CMS guidance, the documentation in the patient’s IRF
medical record must demonstrate a reasonable expectation that the following criteria were met at the time of admission to the IRF. The patient must:
- Require active and ongoing intervention of multiple therapy disciplines (Physical
Therapy [PT], Occupational Therapy [OT], Speech-Language Pathology [SLP], or
prosthetics/orthotics), at least one of which must be PT or OT; - Require an intensive rehabilitation therapy program, generally consisting of:
◦ 3 hours of therapy per day at least 5 days per week; or
◦ In certain well-documented cases, at least 15 hours of intensive rehabilitation
therapy within a 7-consecutive day period, beginning with the date of admission; - Reasonably be expected to actively participate in, and benefit significantly
from, the intensive rehabilitation therapy program (the patient’s condition and
functional status are such that the patient can reasonably be expected to make
measurable improvement, expected to be made within a prescribed period of time
and as a result of the intensive rehabilitation therapy program, that will be of practical value to improve the patient’s functional capacity or adaptation to impairments); - Require physician supervision by a rehabilitation physician, with face-to-face
visits at least 3 days per week to assess the patient both medically and functionally
and to modify the course of treatment as needed; and - Require an intensive and coordinated interdisciplinary team approach to the
delivery of rehabilitative care.
Did you notice how often the word “generally” or “reasonably” was used? Because the standard for an IRF stay is subjective. In fact, I would wager a bet that if I reviewed the same documentation as the Palmetto auditors did, that I could make a legal argument that the opposite conclusion should have been drawn. I do it all the time. This is the reason that so many audits are easily overturned…they are subjective!
Therefore, when you get an audit result, such as the ones referenced above:
APPEAL! APPEAL! APPEAL!
Medicare Audits – TPE Audits Are Here, But For How Long?
The Center for Medicare and Medicaid Services (CMS) announced the expansion of Targeted Probe and Educate (TPE) audits. At first glance, this appears to be fantastic news coming on the heels of so much craziness at Health and Human Services (HHS). We have former-HHS Secretary Price flying our tax dollars all over. Dr. Don Wright stepping up as our new Secretary. The Medicare appeal backlog fiasco. The repeal and replace Obamacare bomb. Amidst all this tomfoolery, health care providers are still serving Medicare and Medicaid patients, reimbursement rates are in the toilet, which drives down quality and incentivizes providers to not accept Medicare or Medicaid (especially Caid), and providers are undergoing “Audit Alphabet Soup.” I actually had a client tell me that he receives audit letters requesting documents and money every single week from a plethora of different organizations.
So when CMS announced that it was broadening its TPE audits, it was a sigh of relief for many providers. But will TPE audits be the benign beasts they are purporting to be?
What is a TPE audit? (And – Can We Have Anymore Acronyms…PLEASE!)
CMS says that TPE audits are benevolent. CMS’ rhetoric indicates that these audits should not cause the toner to run out from overuse. CMS states that TPE audits will involve “the review of 20-40 claims per provider, per item or service, per round, for a total of up to three rounds of review.” See CMS Announcement. The idea behind the TPE audits (supposedly) is education, not recoupments. CMS states that “After each round, providers are offered individualized education based on the results of their reviews. This program began as a pilot in one MAC jurisdiction in June 2016 and was expanded to three additional MAC jurisdictions in July 2017. As a result of the successes demonstrated during the pilot, including an increase in the acceptance of provider education as well as a decrease in appealed claims decisions, CMS has decided to expand to all MAC jurisdictions later in 2017.” – And “later in 2017” has arrived. These TPE audits are currently being conducted nationwide.
Below is CMS’ vision for a TPE audit:

Clear? As mud?
The chart does not indicate how long the provider will have to submit records or how quickly the TPE auditors will review the documents for compliance. But it appears to me that getting through Round 3 could take a year (this is a guess based on allowing the provider 30 days to gather the records and allowing the TPE auditor 30 days to review).
Although the audit is purportedly benign and less burdensome, a TPE audit could take a whole year or more. Whether the audit reviews one claim or 20, having to undergo an audit of any size for a year is burdensome on a provider. In fact, I have seen many companies having to hire staff dedicated to responding to audits. And here is the problem with that – there aren’t many people who understand Medicare/caid medical billing. Providers beware – if you rely on an independent biller or an electronic medical records program, they better be accurate. Otherwise the buck stops with your NPI number.
Going back to CMS’ chart (above), notice where all the “yeses” go. As in, if the provider is found compliant , during any round, all the yeses point to “Discontinue for at least 12 months.” I am sure that CMS thought it was doing providers a favor, but what that tells me is the TPE audit will return after 12 months! If the provider is found compliant, the audit is not concluded. In fact, according to the chart, the only end results are (1) a referral to CMS for possible further action; or (2) continued TPE audits after 12 months. “Further action” could include 100% prepayment review, extrapolation, referral to a Recovery Auditor, or other action. Where is the outcome that the provider receives an A+ and is left alone??
CMS states that “Providers/suppliers may be removed from the review process after any of the three rounds of probe review, if they demonstrate low error rates or sufficient improvement in error rates, as determined by CMS.”
I just feel as though that word “may” should be “will.” It’s amazing how one word could change the entire process.
Knicole Emanuel Featured on Hospital Finance Podcast – Medicare Appeal Backlog (Legal Update)
On September 6, 2017, I appeared on the Besler Hospital Finance Podcast regarding:
Update on the Medicare appeals backlog [PODCAST]
Feel free to listen to the podcast, download it, and share with others!
SB 257 – A New Death Sentence for NC Medicaid Providers!
Buried within the Senate Appropriations Act of 2017 (on pages 189-191 of 361 pages) is a new and improved method to terminate Medicaid providers. Remember prepayment review? Well, if SB 257 passes, then prepayment review just…
got…
bigger.
Prepayment review is allowed per N.C. Gen. Stat. 108C-7. See my past blogs on my opinion as to prepayment review. “NC Medicaid: CCME’s Comedy of Errors of Prepayment Review” “NC Medicaid and Constitutional Due Process.”
N.C. Gen. Stat. 108C-7 states, “a provider may be required to undergo prepayment claims review by the Department. Grounds for being placed on prepayment claims review shall include, but shall not be limited to, receipt by the Department of credible allegations of fraud, identification of aberrant billing practices as a result of investigations or data analysis performed by the Department or other grounds as defined by the Department in rule.” Getting placed on prepayment review is not appealable. Relief can be attainable. See blog. (With a lawyer and a lot of money).
Even without the proposals found within SB 257, being placed on prepayment review is being placed in a torture chamber for providers.
With or without SB 257, being placed on prepayment review results in the immediate withhold of all Medicaid reimbursements pending the Department of Health and Human Services’ (DHHS) contracted entity’s review of all submitted claims and its determination that the claims meet criteria for all rules and regulations. If the majority of your reimbursements come from Medicaid, then an immediate suspension of Medicaid funds can easily put you out of business.
With or without SB 257, in order to get off prepayment review, you must achieve 70% accuracy (or clean claims) for three consecutive months. Think about that statement – The mere placement of you on prepayment review means that, according to the standard for being removed from prepayment review, you will not receive your reimbursements for, at least, three months. How many of you could survive without getting paid for three months. But that’s not the worst of it, the timing and process of prepayment review – meaning the submission of claims, the review of the claims, the requests for more documentation, submission of more documents, and the final decision – dictates that you won’t even get an accuracy rating the first, maybe even the second month. If you go through the prepayment review process, you can count on no funding for four to five months, if you are over 70% accurate the first three months. How many of you can sustain your company without getting paid for five months? How about 24 months, which is how long prepayment review can last?
The prepayment review process: (legally, which does not mean in reality)
Despite your Medicaid funds getting cut off, you continue to provide Medicaid services to your recipients (You also continue to pay your staff and your overhead with gummy bears, rainbows, and smiles). – And, according to SB 257, if your claims submissions decrease to under 50% of the prior three months before prepayment review – you automatically lose. In other words, you are placed on prepayment review. Your funding is suspended (with or without SB 257). You must continue to provide services without any money (with or without SB 257) and you must continue to provide the same volume of services (if SB 257 passes).
So, you submit your claims.
The Department of Health and Human Services (DHHS) or its contracted vendor shall process all clean claims submitted for prepayment review within 20 calendar days of submission by the provider. “To be considered by the Department, the documentation submitted must be complete, legible, and clearly identify the provider to which the documentation applies. If the provider failed to provide any of the specifically requested supporting documentation necessary to process a claim pursuant to this section, the Department shall send to the provider written notification of the lacking or deficient documentation within 15 calendar days of receipt of such claim the due date of requested supporting documentation. The Department shall have an additional 20 days to process a claim upon receipt of the documentation.”
Let’s look at an example:
You file your claim on June 1, 2017.
DHHS (or contractor) determines that it needs additional documentation. On June 16, 2017, DHHS sends a request for documentation, due by July 6, 2017 (20 days later).
But you are on the ball. You do not need 20 days to submit the additional documents (most likely, because you already submitted the records being requested). You submit additional records on June 26, 2017 (within 10 days).
DHHS has until July 16, 2017, to determine whether the claim is clean. A month and a half after you submit your claim, you will be told whether or not you will be paid, and that’s if you are on the ball.
Now imagine that you submit 100 claims per week, every week. Imagine the circular, exponential effect of the continual, month-and-a-half review for all the claims and the amount of documents that you are required to submit – all the while maintaining the volume of claims of, at least over 50% of your average from the three prior months before prepayment review.
Maintaining at least 50% of the volume of claims that you submitted prior to being placed on prepayment review is a new addition to the prepayment review torture game and proposed in SB 257.
If SB 257 does not pass, then when you are placed on prepayment review and your funding is immediately frozen, you can decrease the volume of claims you submit. It becomes necessary to decrease the volume of claims for many reasons. First, you have no money to pay staff and many staff will quit; thus decreasing the volume of claims you are able to provide. Second, your time will be consumed with submitting documents for prepayment review, receiving additional requests, and responding to the additional requests. I have had a client on prepayment review receive over 100 requests for additional documents per day, for months. Maintaining organization and a record of what you have or have not submitted for which Medicaid recipient for which date of service becomes a full-time job. With your new full-time job as document submitter, your volume of services decreases.
Let’s delve into the details of SB 257 – what’s proposed?
SB 257’s Proposed Torture Tactics
The first Catherine’s Wheel found in SB 257 is over 50% volume. Or you will be terminated.
As discussed, SB 257 requires to maintain at least 50% of the volume of services you had before being placed on prepayment review. Or you will be terminated.
Another heretics fork that SB 257 places in the prepayment review torture chamber is punishment for appeal.
SB 257 proposes that you are punished for appealing a termination. If you fail to meet the 70% accuracy for three consecutive months, then you will be terminated from the Medicaid program. However, with SB 257, if you appeal that termination decision, then “the provider shall remain on prepayment review until the final disposition of the Department’s termination or other sanction of the provider.” Normally when you appeal an adverse determination, the adverse determination is “stayed” until the litigation is over.
Another Iron Maiden that SB 257 proposes is exclusion.
SB 257 proposes that if you are terminated “the termination shall reflect the provider’s failure to successfully complete prepayment claims review and shall result in the exclusion of the provider from future participation in the Medicaid program.” Even if you voluntarily terminate. No mulligan. No education to improve yourself. You never get to provide Medicaid services again. The conical frame has closed.
Another Guillotine that SB 257 proposes is no withhold of claims.
SB 257 proposes that if you withhold claims while you are on prepayment review. “any claims for services provided during the period of prepayment review may still be subject to review prior to payment regardless of the date the claims are submitted and regardless of whether the provider has been taken off prepayment review.”
Another Judas Chair that SB 257 proposes is no new evidence.
SB 257 proposes that “[i]f a provider elects to appeal the Department’s decision to impose sanctions on the provider as a result of the prepayment review process to the Office of Administrative Hearings, then the provider shall have 45 days from the date that the appeal is filed to submit any documentation or records that address or challenge the findings of the prepayment review. The Department shall not review, and the administrative law judge shall not admit into evidence, any documentation or records submitted by the provider after the 45-day deadline. In order for a provider to meet its burden of proof under G.S. 108C-12(d) that a prior claim denial should be overturned, the provider must prove that (i) all required documentation was provided at the time the claim was submitted and was available for review by the prepayment review vendor and (ii) the claim should not have been denied at the time of the vendor’s initial review.”
The prepayment review section of SB 257, if passed, will take effect October 1, 2017. SB 257 has passed the Senate and now is in the House.
Medicare/Caid Audits: Urine Testing Under Fire!!
I have blogged about peeing in a cup before…but we will not be talking about dentists in this blog. Instead we will be discussing pain management physicians and peeing in a cup.
Pain management physicians are under intense scrutiny on the federal and state level due to increased urine testing. But is it the pain management doctors’ fault?
When I was little, my dad and I would play catch with bouncy balls. He would always play a dirty little trick, and I fell for it every time. He would toss one ball high in the air. While I was concentrating on catching that ball, he would hurl another ball straight at me, which, every time, smacked into me – leaving me disoriented as to what was happening. He would laugh and laugh. I was his Charlie Brown, and he was my Lucy. (Yes, I have done this to my child).
The point is that it is difficult to concentrate on more than one thing. When the Affordable Care Act (ACA) came out, it was as if the federal government wielded 500, metaphoric, bouncy balls at every health care provider. You couldn’t comprehend it in its entirety. There were different deadlines for multiple changes, provider requirements, employer requirements, consumer requirements…it was a bloodbath! [If you haven’t seen the brothers who trick their sister into thinking it’s a zombie apocalypse, you have to watch it!!]
A similar “metaphoric ball frenzy” is occurring now with urine testing, and pain management physicians make up the bulk of prescribed urine testing. The urine testing industry has boomed in the past 4-5 years. This could be caused by a number of factors:
- increase use of drugs (especially heroine and opioids),
- the tightening of regulations requiring physicians to monitor whether patients are abusing drugs,
- increase of pain management doctors purchasing mass-spectrometry machines and becoming their own lab,
- simply more people are complaining of pain, and
- the pharmaceutical industry’s direct-to-consumer advertising (DTCA).
Medicare’s spending on 22 high-tech tests for drugs of abuse hit $445 million in 2012, up 1,423% in five years. “In 2012, 259 million prescriptions were written for opioids, which is more than enough to give every American adult their own bottle of pills.” See article.
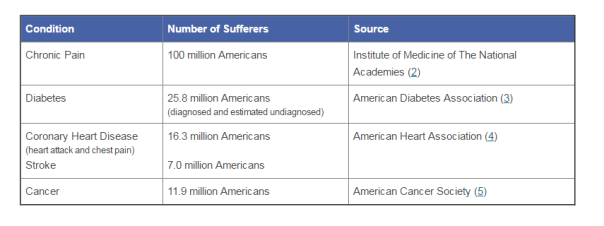
According to the American Association of Pain Management, pain affects more Americans than diabetes, heart disease and cancer combined. The chart below depicts the number of chronic pain sufferers compared to other major health conditions.
In the world of Medicare and Medicaid, where there is profit being made, the government comes a-knockin’.
But should we blame the pain management doctors if recent years brought more patients due to increase of drug use? The flip side is that we do not want doctors ordering urine tests unnecessarily. But aren’t the doctors supposed to the experts on medical necessity??? How can an auditor, who is not a physician and never seen the patient opine to medical necessity of a urine test?
The metaphoric ball frenzy:
There are so many investigations into urine testing going on right now.
Ball #1: The machine manufacturers. A couple of years ago, Carolina Liquid Chemistries (CLC) was raided by the federal government. See article. One of the allegations was that CLC was misrepresenting their product, a urinalysis machine, which caused doctors to overbill Medicare and Medicaid. According to a source, the federal government is still investigating CLC and all the physicians who purchased the urinalysis machine from CLC.
Ball #2: The federal government. Concurrently, the federal government is investigating urine testing billed to Medicare. In 2015, Millennium Health paid $256 million to resolve alleged violations of the False Claims Act for billing Medicare and Medicaid for medically unnecessary urine drug and genetic testing. I wonder if Millennium bought a urinalysis machine from CLC…
Ball #3: The state governments. Many state governments are investigating urine testing billed to Medicaid. Here are a few examples:
New Jersey: July 12, 2016, a couple and their diagnostic imaging companies were ordered to pay more than $7.75 million for knowingly submitting false claims to Medicare for thousands of falsified diagnostic test reports and the underlying tests.
Oklahoma: July 10, 2016, the Oklahoma attorney general’s office announced that it is investigating a group of laboratories involved in the state’s booming urine testing industry.
Tennessee: April 2016, two lab professionals from Bristol, Tenn., were convicted of health care fraud in a scheme involving urine tests for substance abuse treatments.
If you are a pain management physician, here are a few recommendations to, not necessarily avoid an audit (because that may be impossible), but recommendations on how to “win” an audit:
- Document, document, document. Explain why the urine test is medically necessary in your documents. An auditor is less likely to question something you wrote at the time of the testing, instead of well after the fact.
- Double check the CPT codes. These change often.
- Check your urinalysis machine. Who manufactured it? Is it performing accurately?
- Self-audit
- Have an experienced, knowledgeable, health care attorney. Do not wait for the results of the audit to contact an attorney.
And, perhaps, the most important – Do NOT just accept the results of an audit. Especially with allegations involving medical necessity…there are so many legal defenses built into regulations!! You turn around and throw a bouncy ball really high – and then…wallop them!!
Health Care Integration: A Glimpse Into My Crystal Ball
Throughout the history of health care, payors and payees of Medicare/caid have existed in separate silos. In fact, the two have combated – the relationship has not always been stellar.
Looking into my crystal ball; however, all will not be as it is now [that’s clear as mud!].
Now, and in the upcoming years, there will be a massive shift to integrate payors and payees under the same roof. Competition drives this movement. So does the uncertainty in the health care market. This means that under one umbrella may be the providers and the paying entities.
Why is this a concern? First – Any healthcare entity that submits claims to the federal government, whether it be a provider or payor, must comply with the fraud and abuse statutes. As such, there is a potential to run afoul of federal and state regulations regulating the business of health care. Payors know their rules; providers know their rules…And those rules are dissimilar; and, at times, conflicting. The opportunity to screw up is endemic.
Second – With the new responsibilities mandated by the Yates Memo, these new relationships could create awkward situations in which the head of the payor department could have knowledge (or should have knowledge) of an [alleged] overpayment, but because of the politics at the company or self-interest in the preservation of his or her career, the head may not want to disclose such overpayment. With the 60-day rule, the head’s hesitation could cost the company.
Let’s investigate:
The Affordable Care Act (ACA) reinvented health care in so many ways. Remember, the ACA is supposed to be self-funding. Taxes were not to increase due to its inception. Instead, health care providers fund the ACA through post payment and prepayment audits, ZPIC audits, CERTs, MFCU, MICs, RACs, and PERMs.
The ACA also made a whole new commercially-insured population subject to the False Claims Act. False statements are now being investigated in connection with Medical Loss Ratios, justifications for rate increases, risk corridor calculations, or risk adjustment submissions.
CMS imposes a duty to detect fraud, waste, and abuse (FWA). But what if you’re looking at your own partners?

The chart above depicts “old school” Medicare payment options for physicians and other health care providers. In our Brave New World, the arrows will be criss-crossed (applesauce), because when the payors and the payees merge, the reimbursements, the billing, and the regulatory supervision will be underneath the same roof. It’ll be the game of “chicken” taken to a whole new level…with prison and financial penalties for the loser.
Since 2011, kickback issues have exponentially grown. The Anti-Kickback Statute makes it a criminal offense for a provider to give “remuneration” to a physician in order to compensate the physician for past referrals or to induce future referrals of patients to the provider for items or services that are reimbursed, in whole or in part, by Medicare or Medicaid.
Imagine when payors and payees are owned by the same entity! Plus, the ACA amended the kickback statutes to eliminate the prong requiring actual knowledge or intent. Now you can be convicted of anti kickback issues without any actual knowledge it was ever occurring!!
Now we have the “one purpose test,” which holds that a payment or offer of remuneration violates the Anti-Kickback Statute so long as part of the purpose of a payment to a physician or other referral source by a provider or supplier is an inducement for past or future referrals. United States v. Borrasi, 2011 WL 1663373 (7th Cir. May 4, 2011).
There are statutory exceptions. But these exceptions differ depending on whether you are a payor or payee – see the potential criss-cross applesauce?
And, BTW, which types of health care services are bound by the anti kickback statutes?
- Clinical laboratory services;
- Physical therapy services;
- Occupation therapy services;
- Radiology services (including MRIs, Ultrasounds, and CAT scans);
- Radiation therapy and supplies;
- Durable medical equipment and supplies;
- Parenteral and enteral nutrients, equipment, and supplies;
- Prosthetics, orthotics, and prosthetic devices and supplies;
- Home health services;
- Outpatient prescription drugs; and
- Inpatient and outpatient hospital services.
Imagine a building. Inside is a primary care physician (PCP), a pediatrician, a home health agency, and a psychiatrist. Can the PCP refer to the home health agency? Can a hospital refer to a home care agency? What if one of the Board of Directors sit on both entities?
The keys to avoiding the anti kickback pitfalls is threefold: (1) fair market value (FMV); (2) arm’s length transactions; and (3) money cannot be germane to referrals.
However, there is no one acceptable way to determine FMV. Hire an objective appraiser. While hiring an objective appraiser does not establish accuracy, it can demonstrate a good faith attempt.
Number One Rule for Merging/Acquiring/Creating New Partnerships in our new Brave New World of health care?
Your attorney should be your new BFF!! (Unless she already is).
Another Win for the Good Guys! Federal Preliminary Injunction Granted!!
I do not believe that I have been more excited to post a blog than I am right now. For the past two weeks, an associate DeeDee Murphy and I have been in trial in Albuquerque, New Mexico. For those of you who do not know about the Draconian, governmental upheaval of the 15 behavioral health care companies in New Mexico, see blog. And blog. And documentary.
Going back to what it is that I am so excited to share…
A federal preliminary injunction is rare. It is about as rare as rocking horse poo. But when I met Dr. B, I knew I had to try. Poo or not. Dr. B is a geneticist, who accepts Medicaid. Her services are essential to her patients, who receive ongoing, genetic counseling from her. 70% of her practice comprised of Medicaid recipients.
You see, when Dr. B came to me, she had been represented by legal counsel for over two years but had received no recourse at all. For two years she had retained counsel to fight for her Medicaid contract with the State of Indiana, and for two years, she had no Medicaid contract to render services. For the previous 2 years, Dr. B had been subject to prepayment review and paid nothing – or next to nothing…certainly not enough to pay expenses.
When I met Dr. B, she had not been paid for two years. She continued to render medically necessary services, but she received no reimbursement. She had exhausted all her loans, her credit limit, and even borrowed money from family. She had been forced to terminate staff. Dr. B was on the brink of financial and career ruin. She was about to lose the company and work that she had put over 40 years into. Since her company’s revenue consisted of over 70% Medicaid without Medicaid reimbursements, her company could not survive.
Yet, she continued to provide services to her patients. She is a saint. But she was about to be an unemployed, financially-ruined saint, whose sainthood could not continue.
On December 10, 2015, we filed a Motion for Preliminary Injunction in the Northern District of Indiana requesting that the Court enjoin the Indiana Medicaid agency (“FSSA”) from terminating Dr. B from the Medicaid program and from continuing to suspend the money owed to her for the past two year period that she had been subject to prepayment review.
Senior counsel, Josh Urquhart, from our Denver office, and I attended and argued on behalf of Dr. B in a 5-day trial from January 19-25, 2016.
On April 14, 2016, in a 63-page opinion, our preliminary injunction enjoining Indiana from terminating Dr. B from Medicaid was GRANTED. Dr. B is back in the Medicaid program!!!!!
The rocking horse poo is rampant!
This is not just a win for Dr. B. This is a win for all her Medicaid patients, as well. Two mothers with children-patients of Dr. B testified as to the fact that their children rely heavily on Dr. B. Both testified that without Dr. B their children would be irreparably harmed.
When Dr. B informed her former attorneys that she was hiring me, an attorney from North Carolina, those attorneys told Dr. B that “anyone who tells that they can get a federal preliminary injunction is blowing smoke up your ass.” [Pardon the cuss word – their words, not mine]. To which I would like to say, “[insert raspberry], here’s your smoke!”
A preliminary injunction is an extraordinary and drastic remedy, which is why it is rare. However, rare objects exist. The plaintiff must show the court that he/she has a reasonable likelihood of success on the merits, no adequate remedy at law, and irreparable harm absent the injunction. I felt that we had these criteria covered in Dr. B’s case.
The Court agreed with our contention that FSSA’s without cause termination violates her patients’ freedom to choose their provider. This is a big deal!
In our arguments to the Court, we relied heavily on Planned Parenthood of Indiana. We argued that Indiana’s without cause termination was merely a “business decision” and was not germane to Dr. B’s qualifications. As her qualifications remained intact, to disallow Dr. B from providing medically necessary services violates the patients’ freedom to choose their providers.
The Court held that FSSA “must rescind its without cause termination of Dr. B and reinstate her Medicaid provider agreement until this Court reaches a final decision.”
Even rocking horses poo every now and then.


