Monthly Archives: July 2016
Former mental health providers take fight over Medicaid funds to lawmakers
Loyal followers will remember the behavioral health care debacle that happened in New Mexico in June 2013. See blog and blog and blog. Basically, the State of New Mexico accused 15 behavioral health care companies of credible allegations of fraud and immediately froze all the companies’ Medicaid reimbursements. These 15 companies comprised 87.5% of New Mexico’s behavioral health providers. The companies were forced to close their doors. Hundreds of people lost their jobs. Hundreds of thousands of Medicaid recipients no longer received their medically necessary mental health and substance abuse services. It really was and is such a sad tragedy.
Now, more than 3 years later, the consequences of that payment suspension still haunts those providers. Once they were exonerated of fraud by the Attorney General, the single state entity, Human Services Department (HSD), is now accusing them – one by one – of alleged overpayments. These alleged overpayments are extrapolated. So 10 claims for $600 turns into $2 million. See blog.
I will leave Saturday the 30th of July to fly to Albuquerque, NM, to defend one of those behavioral health care providers in administrative court. The trial is scheduled to last two weeks.
Below is a great article from today’s The Santa Fe New Mexican about this:
By: Justin Horwath
ALBUQUERQUE — Executives of three former mental health agencies told state lawmakers Wednesday that they are still fighting the state’s determination that they overbilled Medicaid, and they are expected to repay millions of dollars, even after they have been cleared of criminal wrongdoing.
“Three years after the fact, and we are still plodding through this,” Shannon Freedle, who was an executive with the now-defunct Teambuilders Counseling Services in Santa Fe, told lawmakers on the Health and Human Services Committee during a hearing in Albuquerque. He was referring to allegations in June 2013 against 15 mental health providers that led to a statewide Medicaid service shake-up.
Along with Freedle, executives of the Santa Fe-based Easter Seals El Mirador and Albuquerque-based Hogares Inc. testified about the New Mexico Human Services Department’s continued claims of Medicaid overpayments long after the state Attorney General’s Office announced it found no evidence that any of the providers had committed fraud and many of the firms have shut down.
Some of the providers, meanwhile, say the state’s former Medicaid claims contractor, OptumHealth New Mexico, still owes them millions of dollars in back payments for treating patients before the shake-up. A group of behavioral health providers, including Teambuilders, Easter Seals and Hogares, filed a lawsuit against OptumHealth in state District Court in June. OptumHealth also faces at least three other lawsuits filed this year, accusing it of Medicaid fraud.
State Rep. Bill O’Neill, D-Albuquerque, called the Human Services Department’s actions “outrageous on so many levels.”
Rep. Christine Trujillo, also an Albuquerque Democrat, called for the resignation of Human Services Department Cabinet Secretary Brent Earnest and for “criminal charges to be pressed because this isn’t human error anymore — this is actually criminal behavior.” She is the second member of the committee to call for Earnest to step down.
No Republicans on the bipartisan committee were at the presentation.
Earlier Wednesday — at a news conference in Albuquerque promoting the Martinez administration’s efforts to tackle New Mexico’s drug abuse epidemic — Gov. Susana Martinez made a rare public comment about the decision in June 2013 to freeze Medicaid payments to the 15 mental health providers on allegations they had defrauded Medicaid, the state and federal program that provides health care to low-income residents. The state brought in five Arizona firms to replace the New Mexico providers, but three of them have since left the state, citing financial losses
Martinez said the decision to freeze the Medicaid payments “was recommended by the federal government.”
“But the patients were continued to be serviced and their services were not interrupted,” she said, “unless they decided on their own that they wanted to not continue.”
Asked to clarify Martinez’s statement about the federal government’s role in the Medicaid payment freeze, Michael Lonergan, the governor’s spokesman, said in an email that Martinez was “referencing federal law, which calls for the state to suspend payments and investigate any credible allegations of fraud.”
Federal law gave the state the option to freeze Medicaid payments but didn’t require it.
Kyler Nerison, a spokesman for the Human Services Department, defended the agency’s efforts to pursue the return of funds allegedly overpaid to the former Medicaid providers, saying in an email that the “Attorney General’s limited review of the agencies that had their payments suspended found thousands of cases of billing errors and other regulatory violations.
“Medicaid dollars should be used to help the people who need it most, and if these politicians want to turn a blind-eye to that kind of waste and abuse, that’s solely on them,” Nerison said. “The Human Services Department will continue working to recoup the misspent and overbilled Medicaid dollars as we continue to help more New Mexicans than ever before in both Medicaid and behavioral health services.”
Freedle said he will attend a Human Services Department hearing next week to contest the agency’s claim that Teambuilders owes the state $2.2 million. At issue is the agency’s use of extrapolation to determine the figure of the alleged overbilling. The agency pointed to 12 allegedly errant claims Teambuilders had made to OptumHealth requesting Medicaid reimbursements worth a total of $728.
But Freedle said the Human Services Department used overpayments found in a small sample of claims and multiplied the amount by 3,000 to determine overbilling over a longer period of time, without proving such billing errors occurred. An investigation by the Attorney General’s Office, which found no evidence of criminal fraud, also found a smaller error rate.
Patsy Romero, CEO of Easter Seals El Mirador, and Nancy Jo Archer, who was the CEO of Hogares, broke down in tears as they described the Human Services Department’s “fair hearing process.”
“That’s really and truly an oxymoron,” Archer said.
Medicare Fraud: Do MCOs Have Accountability Too?
Dr. Isaac Kojo Anakwah Thompson, a Florida primary care physician, was sentenced in July 2016 to 4 years in prison and a subsequent two years of supervised release. Dr. Thompson pled guilty to health care fraud. He was further ordered to pay restitution in the amount of $2,114,332.33. Ouch!! What did he do?
According to the Department of Justice, Dr. Thompson falsely reported that 387 of his clients suffered from ankylosing spondylitis when they did not.
Question: How does faking a patient’s disease make a physician money???
Answer: Hierarchal condition category (HCC) coding. Wait, what?
Basically, Medicare Advantage assigns HCC coding to each patient depending on the severity of their illnesses. Higher HCC scores equals substantially higher monthly capitation payments from Medicare to the managed care organization (MCO). In turn, the MCO will pay physicians more who have more extremely sick patients (higher HCC codes).
Ankylosing spondylitis is a form of arthritis that causes inflammation and damage at the joints; eventually, the inflamed spinal joints can become fused, or joined together so they can’t move independently. It’s a rare disease, affecting 1 in 1000 people. And, importantly, it sports a high HCC code.
In this case, the Office of Inspector General (OIG) found it odd that, between 2006-2010, Dr. Thompson diagnosed 387 Medicare Advantage beneficiaries with ankylosing spondylitis and treated them with such rare disease. To which, I say, if you’re going to defraud the Medicare system, choose common, fabricated diseases (kidding – it’s called sarcasm – I always have to add a disclaimer for people with no humor).
According to the Department of Justice, none or very few of Dr. Thompson’s 387 consumers actually had ankylosing spondylitis.
My issue is as follows: Doesn’t the managed care organization (MCO) share in some of the punishment? Shouldn’t the MCO have to repay the financial benefit it reaped from Dr. Thompson?? Shouldn’t the MCO have a duty to report such oddities?
Let me explain:
In Florida, Humana acted as the MCO. Every dollar that Dr. Thompson received was funneled through Humana. Humana would pay Dr. Thompson a monthly capitation fee from Medicare Advantage based on his patient’s hierarchal condition category (HCC) coding. Increasing even just one patient’s HCC code means more bucks for Dr. Thompson. Remember, according to the DOJ, he increased 387 patients’ HCC codes.
Dr. Thompson reported these diagnoses to Humana, which in turn reported them to Medicare. Consequently, Medicare paid approximately $2.1 million in excess capitation fees to Humana, approximately 80% of which went to Dr. Thompson.
In this case, it is reasonable to expect that Humana had knowledge that Dr. Thompson reported abnormally high HCCs for his patients. For comparison, ankylosing spondylitis has an HCC score of 0.364, which is more than an aortic aneurysm and three times as high as diabetes. Plus, look at the amount of money that the MCO paid Dr. Thompson. Surely, it appeared irregular.
What, if anything, is the MCO’s duty to report physicians with an abnormally high number of high HCC codes? If you have knowledge of someone committing a crime and you do nothing, isn’t that called aiding and abetting?
With the publication of the Yates memo, I expect to see CMS holding MCOs and other state agencies accountable for the actions of its providers. Not to say that the MCOs should actively, independently investigate Medicare/caid fraud, but to notify the Human Services Department (HSD) if abnormalities exist, especially if as blatant as one doctor with 387 patients suffering from ankylosing spondylitis.
The New White Collar Exemptions: The Final Rule, (an exception), and the Possible Consequences
On May 18, 2016, the US Department of Labor (DOL) announced the Final Rule amending the “white collar” overtime exemptions to increase the number of employees eligible for overtime, effective December 1, 2016. Got overtime? There is no phase-in; it is immediately effective on December 1st.
We all know that the Affordable Care Act (ACA) placed heavier burdens on employers with the employer mandate for employee health insurance. But, the burdens didn’t stop with the ACA!! Oh, no! In 2014, President Obama signed an Executive Order directing the Department of Labor to update the regulations defining which white collar workers are protected by the Fair Labor Standards Act (FLSA) minimum wage and overtime standards. How else could we financially burden employers? We could mandate employers pay overtime to salaried workers!!! Oh, we already do? Let’s raise the overtime salary threshold exemptions so more employees receive overtime!!

You ask, “How is the DOL Final Rule on white collar exemptions germane to my health care agency/practice?” Answer: Do you have employees? If yes, the Final Rule is applicable to you. If no, there is no need to read this blog (unless you are a salaried employee and want to receive more overtime).
The new, increased salary threshold for executives, administration, and professionals exemptions swells from $455/week to $913/week or $23,660/year to $47,476/year. The number for the ceiling is actually less than what was proposed by $800/week. These numbers are based on 40th percentile of full-time employees (salaried) in the lowest wage region, which happens to be the South. Don’t get your knickers in a knot.
Furthermore, the exemption for the highly compensated employee will jump from $100,000 to $134,004 (odd number). This number is $12,000 more than the proposed amount. Well, that just dills my pickle!
The Final Rule also requires that the salary threshold for executives, administration, and professionals be reviewed every three years in order to maintain the salary exemption comparable to the 40th percentile of full-time employees (salaried) in the lowest wage census region – the South.
Finally, the salary basis test will be amended to allow employers to use non-discretionary bonuses and incentive payments, such as commissions, to satisfy the requirements up to 10% of the salary threshold.
The allowance of non-discretionary bonuses and incentive payments was meant to soften the blow of the increased salary thresholds. That’s about as useless as a screen door on a submarine/a trapdoor on a canoe.
VERY IMPORTANT EXCEPTION
The Secretary of DOL issued a time-limited non-enforcement policy for providers of Medicaid-funded services for individuals with intellectual or developmental disabilities in residential homes and facilities with 15 or fewer beds. From December 1, 2016 to March 17, 2019, the Department will not enforce the updated salary thresholds.
BUT THE REST OF US BEWARE!!
Do your math!! If the 10% maximum allowance is exceeded, you could find yourself in a world of hurt! We are talking misclassification claims! Also, ensure you know the proper distinctions between discretionary and non-discretionary bonuses!
What likely consequences will arise from this Final Rule? There are a number of possibilities:
- Employers will raise employees’ salaries to the new levels;
- Employers will pay more overtime;
- Employers will convert the salaried employees to hourly;
- Employers will change benefits or other operation costs to compensate for the increased burden.
Well, that’s just lower than a snake’s belly in a wagon rut!
Turning Medicare Into a Premium Support System: Frequently Asked Questions — The Henry J. Kaiser Family Foundation
Premium support is a general term used to describe an approach to reform Medicare that aims to reduce the growth in Medicare spending. These FAQs raise and discuss basic questions about the possible effects of a premium support system for Medicare beneficiaries, the federal budget, health care providers, and private health plans.
Medicare/Caid Audits: Urine Testing Under Fire!!
I have blogged about peeing in a cup before…but we will not be talking about dentists in this blog. Instead we will be discussing pain management physicians and peeing in a cup.
Pain management physicians are under intense scrutiny on the federal and state level due to increased urine testing. But is it the pain management doctors’ fault?
When I was little, my dad and I would play catch with bouncy balls. He would always play a dirty little trick, and I fell for it every time. He would toss one ball high in the air. While I was concentrating on catching that ball, he would hurl another ball straight at me, which, every time, smacked into me – leaving me disoriented as to what was happening. He would laugh and laugh. I was his Charlie Brown, and he was my Lucy. (Yes, I have done this to my child).
The point is that it is difficult to concentrate on more than one thing. When the Affordable Care Act (ACA) came out, it was as if the federal government wielded 500, metaphoric, bouncy balls at every health care provider. You couldn’t comprehend it in its entirety. There were different deadlines for multiple changes, provider requirements, employer requirements, consumer requirements…it was a bloodbath! [If you haven’t seen the brothers who trick their sister into thinking it’s a zombie apocalypse, you have to watch it!!]
A similar “metaphoric ball frenzy” is occurring now with urine testing, and pain management physicians make up the bulk of prescribed urine testing. The urine testing industry has boomed in the past 4-5 years. This could be caused by a number of factors:
- increase use of drugs (especially heroine and opioids),
- the tightening of regulations requiring physicians to monitor whether patients are abusing drugs,
- increase of pain management doctors purchasing mass-spectrometry machines and becoming their own lab,
- simply more people are complaining of pain, and
- the pharmaceutical industry’s direct-to-consumer advertising (DTCA).
Medicare’s spending on 22 high-tech tests for drugs of abuse hit $445 million in 2012, up 1,423% in five years. “In 2012, 259 million prescriptions were written for opioids, which is more than enough to give every American adult their own bottle of pills.” See article.
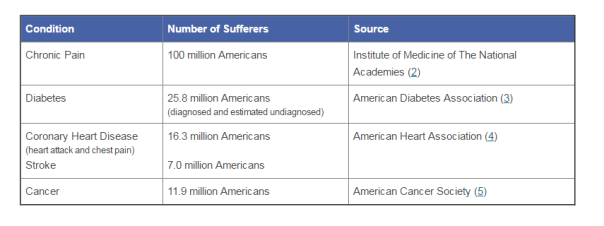
According to the American Association of Pain Management, pain affects more Americans than diabetes, heart disease and cancer combined. The chart below depicts the number of chronic pain sufferers compared to other major health conditions.
In the world of Medicare and Medicaid, where there is profit being made, the government comes a-knockin’.
But should we blame the pain management doctors if recent years brought more patients due to increase of drug use? The flip side is that we do not want doctors ordering urine tests unnecessarily. But aren’t the doctors supposed to the experts on medical necessity??? How can an auditor, who is not a physician and never seen the patient opine to medical necessity of a urine test?
The metaphoric ball frenzy:
There are so many investigations into urine testing going on right now.
Ball #1: The machine manufacturers. A couple of years ago, Carolina Liquid Chemistries (CLC) was raided by the federal government. See article. One of the allegations was that CLC was misrepresenting their product, a urinalysis machine, which caused doctors to overbill Medicare and Medicaid. According to a source, the federal government is still investigating CLC and all the physicians who purchased the urinalysis machine from CLC.
Ball #2: The federal government. Concurrently, the federal government is investigating urine testing billed to Medicare. In 2015, Millennium Health paid $256 million to resolve alleged violations of the False Claims Act for billing Medicare and Medicaid for medically unnecessary urine drug and genetic testing. I wonder if Millennium bought a urinalysis machine from CLC…
Ball #3: The state governments. Many state governments are investigating urine testing billed to Medicaid. Here are a few examples:
New Jersey: July 12, 2016, a couple and their diagnostic imaging companies were ordered to pay more than $7.75 million for knowingly submitting false claims to Medicare for thousands of falsified diagnostic test reports and the underlying tests.
Oklahoma: July 10, 2016, the Oklahoma attorney general’s office announced that it is investigating a group of laboratories involved in the state’s booming urine testing industry.
Tennessee: April 2016, two lab professionals from Bristol, Tenn., were convicted of health care fraud in a scheme involving urine tests for substance abuse treatments.
If you are a pain management physician, here are a few recommendations to, not necessarily avoid an audit (because that may be impossible), but recommendations on how to “win” an audit:
- Document, document, document. Explain why the urine test is medically necessary in your documents. An auditor is less likely to question something you wrote at the time of the testing, instead of well after the fact.
- Double check the CPT codes. These change often.
- Check your urinalysis machine. Who manufactured it? Is it performing accurately?
- Self-audit
- Have an experienced, knowledgeable, health care attorney. Do not wait for the results of the audit to contact an attorney.
And, perhaps, the most important – Do NOT just accept the results of an audit. Especially with allegations involving medical necessity…there are so many legal defenses built into regulations!! You turn around and throw a bouncy ball really high – and then…wallop them!!
Health Care Integration: A Glimpse Into My Crystal Ball
Throughout the history of health care, payors and payees of Medicare/caid have existed in separate silos. In fact, the two have combated – the relationship has not always been stellar.
Looking into my crystal ball; however, all will not be as it is now [that’s clear as mud!].
Now, and in the upcoming years, there will be a massive shift to integrate payors and payees under the same roof. Competition drives this movement. So does the uncertainty in the health care market. This means that under one umbrella may be the providers and the paying entities.
Why is this a concern? First – Any healthcare entity that submits claims to the federal government, whether it be a provider or payor, must comply with the fraud and abuse statutes. As such, there is a potential to run afoul of federal and state regulations regulating the business of health care. Payors know their rules; providers know their rules…And those rules are dissimilar; and, at times, conflicting. The opportunity to screw up is endemic.
Second – With the new responsibilities mandated by the Yates Memo, these new relationships could create awkward situations in which the head of the payor department could have knowledge (or should have knowledge) of an [alleged] overpayment, but because of the politics at the company or self-interest in the preservation of his or her career, the head may not want to disclose such overpayment. With the 60-day rule, the head’s hesitation could cost the company.
Let’s investigate:
The Affordable Care Act (ACA) reinvented health care in so many ways. Remember, the ACA is supposed to be self-funding. Taxes were not to increase due to its inception. Instead, health care providers fund the ACA through post payment and prepayment audits, ZPIC audits, CERTs, MFCU, MICs, RACs, and PERMs.
The ACA also made a whole new commercially-insured population subject to the False Claims Act. False statements are now being investigated in connection with Medical Loss Ratios, justifications for rate increases, risk corridor calculations, or risk adjustment submissions.
CMS imposes a duty to detect fraud, waste, and abuse (FWA). But what if you’re looking at your own partners?

The chart above depicts “old school” Medicare payment options for physicians and other health care providers. In our Brave New World, the arrows will be criss-crossed (applesauce), because when the payors and the payees merge, the reimbursements, the billing, and the regulatory supervision will be underneath the same roof. It’ll be the game of “chicken” taken to a whole new level…with prison and financial penalties for the loser.
Since 2011, kickback issues have exponentially grown. The Anti-Kickback Statute makes it a criminal offense for a provider to give “remuneration” to a physician in order to compensate the physician for past referrals or to induce future referrals of patients to the provider for items or services that are reimbursed, in whole or in part, by Medicare or Medicaid.
Imagine when payors and payees are owned by the same entity! Plus, the ACA amended the kickback statutes to eliminate the prong requiring actual knowledge or intent. Now you can be convicted of anti kickback issues without any actual knowledge it was ever occurring!!
Now we have the “one purpose test,” which holds that a payment or offer of remuneration violates the Anti-Kickback Statute so long as part of the purpose of a payment to a physician or other referral source by a provider or supplier is an inducement for past or future referrals. United States v. Borrasi, 2011 WL 1663373 (7th Cir. May 4, 2011).
There are statutory exceptions. But these exceptions differ depending on whether you are a payor or payee – see the potential criss-cross applesauce?
And, BTW, which types of health care services are bound by the anti kickback statutes?
- Clinical laboratory services;
- Physical therapy services;
- Occupation therapy services;
- Radiology services (including MRIs, Ultrasounds, and CAT scans);
- Radiation therapy and supplies;
- Durable medical equipment and supplies;
- Parenteral and enteral nutrients, equipment, and supplies;
- Prosthetics, orthotics, and prosthetic devices and supplies;
- Home health services;
- Outpatient prescription drugs; and
- Inpatient and outpatient hospital services.
Imagine a building. Inside is a primary care physician (PCP), a pediatrician, a home health agency, and a psychiatrist. Can the PCP refer to the home health agency? Can a hospital refer to a home care agency? What if one of the Board of Directors sit on both entities?
The keys to avoiding the anti kickback pitfalls is threefold: (1) fair market value (FMV); (2) arm’s length transactions; and (3) money cannot be germane to referrals.
However, there is no one acceptable way to determine FMV. Hire an objective appraiser. While hiring an objective appraiser does not establish accuracy, it can demonstrate a good faith attempt.
Number One Rule for Merging/Acquiring/Creating New Partnerships in our new Brave New World of health care?


