Category Archives: Reconsideration Reviews
Fairness in Medicare: Post Payment Review in the Courts of Equity
As children, we say things are or are not fair. But what is fair? In law, fairness is “tried” in the courts of equity rather than law. Equitable estoppel and the defense of laches are arguments made in the courts of equity. Is it fair if you’ve been billing Medicare for services that you were told by CMS was billable and reimburse-able – for years – then, unexpectantly, CMS says, “Hey, providers, what you were told was reimburse-able, actually is not. In fact, providers, even though you relied on our own guidance, we will cease and desist from paying you going forward AND…we are now going back three years to retroactively collect the money that we should never have paid you…”
How is this fair? Yet, many of you have probably encountered RAC or MAC audits and a post payment review. What I described is a post payment review. Let me give you an example of a nationwide, claw-back by CMS to providers.
On January 29, 2020, CMS announced that beginning March 1, 2020, MACs will reject claims for HCPCS code L8679 submitted without an appropriate HCPCS/CPT surgical procedure code. Claims for HCPCS code L8679 billed with an appropriate HCPCS/CPT surgical code will be suspended for medical review to verify that coverage, coding, and billing rules have been met.
At least according to the announcement, it sounded like CMS instructed the MACs to stop reimbursing L8679 going forward, but I read nothing about going back in time to recoup.
In the last few months, my team has been approached by chiropractors and holistic medical providers who received correspondence from a UPIC and their MACs that they owe hundreds of thousands of dollars for L8679 going back three years prior to CMS’ 2020 announcement to cease using the code.
In this particular instance, many of the providers who had been using the L8679 code did so under the direct guidance of CMS, MACs, and other agents over the years. It becomes a fairness question. Should CMS be able to recoup for claims paid for services rendered when CMS had informed the providers it was the correct code for years?
Another factor to consider is that many of these providers are victims of an intentional scheme to sell devices with the false advice that the devices are covered by Medicare. Litigation has already been filed against the company. In a case filed December 6, 2019, in US District Court of the Eastern District of PA, Neurosurgical Care LLC sued Mark Kaiser and his current company, Doc Solutions LLC, claiming that Kaiser’s company falsely marketed the device as being covered by Medicare. Stivax is a “non-narcotic and minimally invasive form of neurostimulation” which is represented as “one of the only FDA approved microchip controlled microstimulation devices for treating back, joint and arthritic pain.”
Recall that, over the years, CMS paid for these approved procedures with no problem. This situation begins to leave the realm of the courts of law and into the court of equity. It becomes an equitable issue. Is there fairness in Medicare?
There may not be fairness, but there is an administrative appeal process for health care providers! Use it! Request redeterminations!
Appealing Adverse Decisions: Should We Reconsider the Medicaid Provider Reconsideration Review?
What if you had to appeal traffic citations through the police officer who pulled you over before you could defend yourself before an impartial judge? That would be silly and a waste of time. I could not fathom a time in which the officer would overturn his/her own decision.
“No, officer, I know you claim that I was speeding, but the speed limit on Hwy 1 had just increased to 65. You were wrong when you said the speed limit was 55.”
“Good catch, citizen. You’re right; I’m wrong. Let’s just rip up this speeding ticket.”
Not going to happen.
The same is true when it comes to decisions by the Department of Health and Human Service (DHHS) to sanction or penalize a Medicaid provider based on alleged provider abuse (otherwise known as documentation errors). If DHHS determines that you owe $800,000 because your service notes are noncompliant, I am willing to bet that, upon its own reconsideration, the decision will be upheld. Asking for reconsideration review from the very same entity that decided the sanction or penalty is akin to doing something over and over and expecting different results (definition of insanity?).
But – are informal reconsideration reviews required by law to fight an adverse decision before you may appear before an administrative law judge?
The reason that you should care whether the reconsideration reviews are required by law is because the process is time consuming, and, often, the adverse determination is in effect during the process. If you hire an attorney, it is an expensive process, but one that you will not (likely) win. Generally, I am adverse to spending time and money on something that will yield nothing.
Before delving into whether reconsideration reviews are required by law, here is my caveat: This issue has not been decided by our courts. In fact, our administrative court has rendered conflicting decisions. I believe that my interpretation of the laws is correct (obviously), but until the issue is resolved legally, cover your donkey (CYA), listen to your attorney, and act conservatively.
Different laws relate to whether the adverse decision is rendered by the DHHS or whether the adverse decision is rendered by a managed care organization (MCO). Thus, I will divide this blog into two sections: (1) reconsiderations to DHHS; and (2) reconsiderations to an MCO.
Appealing DHHS Adverse Determinations
When you receive an adverse decision from DHHS, you will know that it is from DHHS because it will be on DHHS letterhead (master of the obvious).

10A NCAC 22F .0402 states that “(a) Upon notification of a tentative decision the provider will be offered, in writing, by certified mail, the opportunity for a reconsideration of the tentative decision and the reasons therefor. (b) The provider will be instructed to submit to the Division in writing his request for a Reconsideration Review within fifteen working days from the date of receipt of the notice. Failure to request a Reconsideration Review in the specified time shall result in the implementation of the tentative decision as the Division’s final decision.”
As seen above, our administrative code recommends that a Medicaid provider undergo the informal reconsideration review process through DHHS to defend a sanction or penalty before presenting before an impartial judge at the Office of Administrative Hearings (OAH). I will tell you, having gone through hundreds upon hundreds of reconsideration reviews, DHHS does not overturn itself. The Hearing Officers know who pay their salaries (DHHS). The reconsideration review ends up being a waste of time and money for the provider, who must jump through the “reconsideration review hoop” prior to filing a petition for contested case.
Historically, attorneys recommend that provider undergo the reconsideration review for fear that an Administrative Law Judge (ALJ) at OAH would dismiss the case based on failure to exhaust administrative remedies. But upon a plain reading of 10A NCAC 22F .0402, is it really required? Look at the language again. “Will be offered” and “the opportunity for.” And what is the penalty for not requesting a reconsideration review? That the tentative decision becomes final – so you can petition to OAH the final decision.
My interpretation of 10A NCAC 22F .0402 is that the informal reconsideration review is an option, not a requirement.
Now, N.C. Gen. Stat. 150B-22 states that “[i]t is the policy of this State that any dispute between an agency and another person that involves the person’s rights, duties, or privileges, including licensing or the levy of a monetary penalty, should be settled through informal procedures. In trying to reach a settlement through informal procedures, the agency may not conduct a proceeding at which sworn testimony is taken and witnesses may be cross-examined. If the agency and the other person do not agree to a resolution of the dispute through informal procedures, either the agency or the person may commence an administrative proceeding to determine the person’s rights, duties, or privileges, at which time the dispute becomes a “contested case.””
It is clear that our State’s policy is that a person who has a grievance against an agency; i.e., DHHS, attempts informal resolution prior to filing an appeal at OAH. Notice that N.C. Gen. Stat. 150B-22 is applicable to any dispute between “an agency and another person.” “Agency” is defined as “an agency or an officer in the executive branch of the government of this State and includes the Council of State, the Governor’s Office, a board, a commission, a department, a division, a council, and any other unit of government in the executive branch. A local unit of government is not an agency.”
Clearly, DHHS is an “agency,” as defined. But an MCO is not a department; or a board; or a commission; or a division; or a unit of government in the executive branch; or a council. Since the policy of exhausting administrative remedies applies to DHHS, are you required to undergo an MCO’s reconsideration review process?
Appealing an MCO Adverse Determination
When you receive an adverse decision from an MCO, you will know that it is from an MCO because it will be on the MCO’s letterhead (master of the obvious).
For example:

There is a reason that I am emphasizing the letterhead. It is because DHHS contracts with a number of vendors. For example, DHHS contracts with Public Consulting Group (PCG), The Carolina Center for Medical Excellence (CCME), HMS, Liberty, etc. You could get a letter from any one of DHHS’ contracted entities – a letter on their letterhead. For example, you could receive a Tentative Notice of Overpayment on PCG letterhead. In that case, PCG is acting on behalf of DHHS. So the informal reconsideration rules would be the same. For MCOs, on the other hand, we obtained a Waiver from the Center for Medicare and Medicaid Services (CMS) to “waive” certain rules and to create the MCOs. Different regulations apply to MCOs than DHHS. In fact, there is an argument that N.C. Gen. Stat. 150B-22 does not apply to the MCOs because the MCOs are not an “agency.” Confusing, right? I call that job security.
Are you required to undergo the MCO’s internal reconsideration review process prior to filing a petition for contested case at OAH?
Your contract with the MCO certainly states that you must appeal through the MCO’s internal process. The MCO contracts with providers have language in them like this:
Dispute Resolution and Appeals: “The CONTRACTOR may file a complaint and/or appeals as outlined in the LME/PIHP Provider Manual promulgated by LME/PIHP pursuant to N.C. Gen. Stat. 122C-151.3 and as provided by N.C. Gen. Stat. Chapter 108C.”
I find numerous, fatal flaws in the above section. Whoever drafted this section of the contract evidently had never read N.C. Gen. Stat. 122C-151.3, which plainly states in subsection (b) “This section does not apply to LME/MCOs.” Also, the LME/PIHP does not have the legal authority to promulgate – that is a rule-making procedure for State agencies, such as DHHS. The third fatal flaw in the above section is that the LME/MCO Provider Manual is not promulgated and certainly was not promulgated not pursuant to N.C. Gen. Stat. 122C-151.3, does not apply to LME/MCOs.
Just because it is written, does not make it right.
If N.C. Gen. Stat. 150B-22 does not apply to MCOs, because MCOs are not an agency, then the State policy of attempting to resolve disputes through informal methods before going to OAH does not apply.
There is no other statute or rule that requires a provider to exhaust an MCO’s internal review process prior to filing a petition for contested case.
What does that mean IN ENGLISH??
What it means is that the MCOs contract and provider manual that create an informal one or two-step reconsideration process is not required by law or rule. You do not have to waste your time and money arguing to the MCO that it should overturn its own decision, even though the reconsideration review process may be outlined in the provider manual or your procurement contract.
OAH has agreed…and disagreed.
In Person-Centered Partnerships, Inc. v. NC DHHS and MeckLINK, No. 13 DHR 18655, the court found that “[n]either the contractual provisions in Article II, Section 5.b of the Medicaid Contract nor MeckLINK’s “Procedures for implementation of policy # P0-09 Local Reconsideration Policy” states that reconsideration review is mandatory and a prerequisite to filing a contested case.”
In another case, OAH has held that, “[c]ontract provisions cannot override or negate the protections provided under North Carolina law, specifically the appeal rights set forth in N.C. Gen. Stat. Chapter 108C. Giesel, Corbin on Contracts § 88.7, at 595 (2011) (When the law confers upon an individual a right, privilege, or defense, the assumption is that the right, privilege or defense is conferred because it is in the public interest. Thus, in many cases, it is contrary to the public interest to permit the holder of the right, privilege, or defense to waive or to bargain it away. In these situations, the attempted waiver or bargain is unenforceable.”)” Essential Supportive Services, LLC v. DHHS and its Agent Alliance Behavioral Healthcare, No. 13 DHR 20386 (NCOAH) (quoting Yelverton’s Enrichment Services, Inc., v. PBH, as legally authorized contractor of and agent for N.C. Department of Health and Human Services, 13-CVS-11337, (7 March 2014)).
However, most recently, OAH ruled in the opposite way. A provider was terminated from an MCO’s catchment area, and we immediately filed a preliminary injunction to cease the termination. As you can see from the above-mentioned cases, OAH had not considered the reconsideration review mandatory. But, this time, the Judge found that the “contractual provision in [the MCO’s] contract with Petitioner, which provides for a local reconsideration review, is a valid and binding provision within the contract.”
So, again, the law is as clear as two and two adding up to five.
For now, when you are disputing an adverse determination by an MCO requesting a reconsideration review before going to OAH is a good CYA.
Going back to the traffic example at the beginning of the blog, my husband was pulled for speeding a few weeks ago. I was surprised because, generally, he does not speed. He is a usually conscientious and careful driver. When the officer came to his window, he was genuinely confused as to the reason for the stop. In his mind, he was driving 73 mph, only 3 miles over the speed limit. In fact, he had the car on cruise control. Turns out he confused the sign for HWY 70, as a speed limit sign. The speed limit was actually 55 mph.
We did not appeal the decision.
Federal Court Orders HHS to Eliminate Medicare Appeal Backlog!
When you have a Medicare appeal, it is not uncommon for the appeal process to last years and years – up to 3-6 years in some cases. There has been a backlog of approximately 800,000+ Medicare appeals (almost 1 million), which, with no change, would take 11 years to vet.
A Federal Court Judge says – that is not good enough!
Judge James Boasburg Ordered that the Medicare appeal backlog be eliminated in the following stages:
- 30% reduction from the current backlog by Dec. 31, 2017 (approximately a 300,000 case reduction within 1 year);
- 60% reduction from the current backlog by Dec. 31, 2018;
- 90% reduction from the current backlog by Dec. 31, 2019; and
- Elimination of the backlog of cases by Dec. 31, 2020;
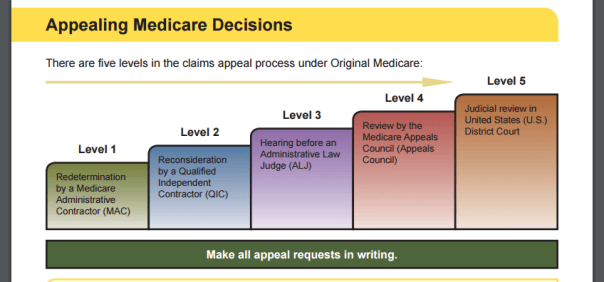
A Medicare appeal has 5 steps. See blog. The backlog is at the Administrative Law Judge (ALJ) level – or, Level 3.
This backlog is largely attributable to the Medicare Recovery Audit Contractor (RAC) programs. In 2010, the federal government implemented the RAC program to recoup allegedly improper Medicare reimbursement payments. The RAC program (for both Medicare and Medicaid) has been criticized for being overly broad and burdensome and “nit picking,” insignificant paperwork errors. See blog.
While the RAC program has recovered a substantial sum of alleged overpayments, concurrently, it has cost health care providers an infinite amount of money to defend the allegations and has left Health and Human Services (HHS) with little funds to adjudicate the number of Medicare appeals, which increase every year. The number of Medicare appeals filed in fiscal year 2011 was 59,600. In fiscal year 2013, that number boomed to more than 384,000. Today, close to 1 million Medicare appeals stand in wait. The statutory adjudication deadline for appeals at the ALJ level is 90 days, yet the average Medicare appeal can last over 546 days.
The American Hospital Association (AHA) said – enough is enough!
AHA sued HHS’ Secretary Sylvia Burwell in 2014, but the case was dismissed. AHA appealed the District Court’s Decision to the Court of Appeals, which reversed the dismissal and gave the District Court guidance on how the backlog could be remedied.
Finally, last week, on December 5, 2016, the District Court published its Opinion and set forth the above referenced mandated dates for eliminating the Medicare appeal backlog.
While, administratively, the case was dismissed, the District Court retained “jurisdiction in order to review the required status reports and rule on any challenges to unmet deadlines.”
In non-legalese, the Court said “The case is over, but we will be watching you and can enforce this Decision should it be violated.”
This is a win for all health care providers that accept Medicare.
RAC Audits: If It Walks Like a Duck and Quacks Like a Duck, It IS a RAC Audit
Recently, hundreds of dentists across North Carolina received Tentative Notices of Overpayment (TNOs) from Public Consulting Group (PCG) demanding recoupment for reimbursements made to dentists who rendered services on Medicaid for Pregnant Women (MPW) eligible recipients. There was no dispute at this hearing that these women were eligible for MPW according to the Department of Health and Human Services’ (DHHS) portal. There was also no dispute that these woman had delivered their babies prior to the date of dental service. So the question becomes: If DHHS informs a dentist that a woman is MPW eligible on the date of the service, does that dentist have an individual and separate burden to determine whether these women are pregnant. And if so, what is it? Have them pee in a cup prior to dental services? See blog, and blog, and blog.
We do not have a definitive answer to the above-posed question, as the Judge has not rendered his decision. However, he did substantially limit these “nameless audits” or “non-RAC” audits to the RAC program limitations. In an Order on our Motion for Partial Summary Judgment, the Administrative Law Judge (ALJ) found that, even if the State does not agree that an audit is a RAC audit, if the audit conducted falls within the definition of a RAC audit, then the audit is a RAC audit.
The reason this is important is because RAC auditors yield such powerful and overwhelming tools against health care providers, the Affordable Care Act (ACA) limits the RAC auditors’ ability to look-back on older claims. For example, even though a provider is, generally, required to maintain records for six (6) years, the federal regulations only allow RAC auditors to look-back three (3) years, unless credible allegations of fraud exist.
Thus, when an auditor reviews documents over three-years-old, I always argue that the review of claims over 3-years-old violates the statute of limitations and federal law.
During hearings, inevitably, the state argues that this particular audit…the one at issue here…is not a RAC audit. The opposing side could no more identify which acronym this audit happens to be, but this audit is not a RAC. “I don’t know what it is, but I know what it’s not!”
Well, an ALJ looked past the rhetoric and pleas by the State that “this is not a RAC” and held that if it walks like a duck and quacks like a duck, then it is a RAC audit and, subsequently, the RAC audit limitations do apply.
In the case for this dentist, Public Consulting Group (PCG) audited claims going back as far as six years! The Department of Health and Human Services’ argument was that this audit is not a RAC audit. So what is it? What makes it NOT a RAC? Because you say so? We all know that PCG has a contract with DHHS to perform RAC audits. Is this audit somehow outside its contractual purview?
So I filed a Motion for Summary Judgment requesting the Judge to throw out all claims outside the three-year look-back period per the RAC limitations.
Lo, and behold, I was right!! (The good guys win again!)
To understand this fully, it is important to first understand what the RAC program is and its intention. (“It depends on what the definition of “is” is”).
Under 42 U.S.C. § 1396a(a)(42):
the State shall—(i) establish a program under which the State contracts (consistent with State law and in the same manner as the Secretary enters into contracts with recovery audit contractors under section 1893(h), subject to such exceptions or requirements as the Secretary may require for purposes of this title or a particular State) with 1 or more recovery audit contractors for the purpose of identifying underpayments and overpayments and recouping overpayments under the State plan and under any waiver of the State plan with respect to all services for which payment is made to any entity under such plan or waiver[].
(emphasis added).
RAC is defined as an entity that “…will review claims submitted by providers of items and services or other individuals furnishing items and services for which payment has been made under section 1902(a) of the Act or under any waiver of the State Plan to identify underpayments and overpayment and recoup overpayments for the States.” 42 CFR § 455.506(a).
Under this definition, PCG is clearly a recovery audit contractor. And the Judge agreed. If it walks like a duck and quacks like a duck, just because the duck protests it is a donkey, it is still a duck. (Hmmmm..wonder how this logic would carry over to the whole transgender bathroom issue…another topic for another blogger…)
RACs must follow certain limitations as outlined in the Code of Federal Regulations. For example, pursuant to 42 C.F.R. § 455.508(f), a Medicaid RAC “must not review claims that are older than 3 years from the date of the claim, unless it receives approval from the State.”
In this particular case, there were 15 claims at issue. Eleven (11) of those claims were outside the three-year look-back period!! With one fell swoop of an ALJ’s signature, we reduced the claims at issue from 15 to 4. Nice!
In DHHS’ Response to our Motion for Partial Summary Judgment, DHHS argued that, in this case, PCG was not acting as a RAC; therefore, the limitations do not apply. In support of such decision, DHHS supplied an affidavit of a DMA employee. She averred that the audit of this particular dentist was not per the RAC program. No rules were cited. No contract in support of her position was provided. Nothing except an affidavit of a DMA employee.
Obviously, it is my opinion that the ALJ was 100% accurate in ruling that this audit was a RAC audit and was limited in scope to a 3-year look-back period.
If it walks like a duck, quacks like a duck, it is not a donkey. No matter how much it pleads that it is, in fact, a donkey!
Remember the Super Bowl Ad of the Puppy, Baby, Monkey?:

That is so NOT ok!
There Is Only One Head Chef in the Medicaid Kitchen, Part Deux!
In a groundbreaking decision published today by the Court of Appeals (COA), the Court smacked down Public Consulting Group’s (PCG), as well as any other contracted entity’s, authority to wield an “adverse decision” against a health care provider. This solidifies my legal argument that I have been arguing on this blog and in court for years!
The Department of Health and Human Services (DHHS) is the “single state agency” charged with managing Medicaid. Federal law requires that that one agency manage Medicaid with no ability to delegate discretionary decisions. Case law in K.C. v. Shipman upheld the federal law. See blog.
Yet, despite K.C. v. Shipman, decided in 2013, in Court, DHHS continued to argue that it should be dismissed from cases in which a contracted vendor rendered the adverse decision to recoup, terminate, or suspend a health care provider. DHHS would argue that it had no part of the decision to recoup, terminate, or suspend, that K.C. Shipman is irrelevant to health care provider cases, and that K.C. v. Shipman is only pertinent to Medicaid recipient cases, to which I countered until I was “blue in the face” is a pile of horse manure.
DHHS would argue that my interpretation would break down the Medicaid system because DHHS cannot possibly review and discern whether every recoupment, termination, and/or suspension made by a contracted vendor was valid (my words, not theirs). DHHS argued that it simply does not have the manpower, plus if it has the authority to contract with a company, surely that company can determine the amount of an alleged overpayment…WRONG!!
In fact, in DHHS v. Parker Home Care, LLC, the COA delineates the exact process for the State determining an overpayment with its contracted agent PCG.
- DHHS may enter into a contract with a company, such as PCG.
- A private company, like PCG, may perform preliminary and full investigations to collect facts and data.
- PCG must submit its findings to DHHS, and DHHS must exercise its own discretion to reach a tentative decision from six options (enumerated in the NC Administrative Code).
- DHHS, after its decision, will notify the provider of its tentative decision.
- The health care provider may request a reconsideration of the tentative decision within 15 days.
- Failure to do so will transform the tentative decision into a final determination.
- Time to appeal to OAH begins upon notification of the final determination by DHHS (60 days).
Another interesting part of this decision is that the provider, Parker Home Care, received the Tentative Notice of Overpayment (TNO) in 2012 and did nothing. The provider did not appeal the TNO.
However, because PCG’s TNO did not constitute a final adverse decision by DHHS (because PCG does not have the authority to render a final adverse decision), the provider did not miss any appeal deadline. The final adverse decision was determined to be DHHS’ action of suspending funds to collect the recoupment, which did not occur until 2014…and THAT action was timely appealed.
The COA’s message to private vendors contracted with DHHS is crystal clear: “There is only one head chef in the Medicaid kitchen.”
Medicare Appeal Backlog: Tough Tooties!…Unless…[Think Outside the Box!]
When you are accused of a $12 million dollar overpayment by Medicare, obviously, you appeal it.But do you expect that appeal to take ten years or longer? Are such long, wait periods allowed by law? That is what Cumberland Community Hospital System, Inc. (Cape Fear) discovered in a 4th Circuit Court of Appeals Decision, on March 7, 2016, denying a Writ of Mandamus from the Court and refusing to order the Secretary of Health and Human Services (HHS) Burwell to immediately adjudicate Cape Fear’s Medicare appeals to be heard within the Congressional requirement that appeals be heard and decided by Administrative Law Judges (ALJs) within 90 days.
According to the Center for Medicare and Medicaid Services‘ (CMS) website, an “ALJ will generally issue a decision within 90 days of receipt of the hearing request. Again, according to CMS’ website, this time frame may be extended for a variety of reasons including, but not limited to:
- The case being escalated from the reconsideration level
- The submission of additional evidence not included with the hearing request
- The request for an in-person hearing
- The appellant’s failure to send a notice of the hearing request to other parties
- The initiation of discovery if CMS is a party.”
In Cape Fear’s case, the Secretary admitted that the Medicare appeal backlog equates to more than 800,000 claims and would, likely, take over 10 years to adjudicate all the claims. Even the 4th Circuit Court, which, ultimately, dismissed Cape Fear’s complaint, agrees with Cape Fear and calls the Medicare appeal backlog “incontrovertibly grotesque.”
Generally, the rule is that if the ALJ does not render a decision after 180 days of the filing of the case, then the provider has the right to escalate the case to the Medicare Appeals Council, which is the 4th step of a Medicare appeal. See blog for more details on the appeal process.
What about after 3,650 days? Get a big pie in the face?
The United States Code is even less vague than CMS’ website. Without question 42 U.S.C. states that for a:
“(1)Hearing by administrative law judge; (A)In general
Except as provided in subparagraph (B), an administrative law judge shall conduct and conclude a hearing on a decision of a qualified independent contractor under subsection (c) of this section and render a decision on such hearing by not later than the end of the 90-day period beginning on the date a request for hearing has been timely filed.”
(emphasis added). And, BTW, subsection (B) is irrelevant here. It contemplates when a party moves for or stipulates to an extension past the 90-day period.
So why did Cape Fear lose? How could the hospital lose when federal administrative code specifically spells out mandatory 90-day limit for a decision by an ALJ? Ever heard of a statute with no teeth? [i.e., HIPAA].
No one will be surprised to read that I have my opinions. First, a writ of mandamus was not the legal weapon to wield. It is an antiquated legal theory that rarely makes itself useful in modern law. I remember the one and only time I filed a writ of mandamus in state court in an attempt to hold a State Agency liable for willfully violating a Court’s Order. I appeared before the judge, who asked me, “Do you know how long I have been on this bench?” To which I responded, “Yes, Your Honor, you have been on the bench for X number of years.” He said, “Do you know how many times I have granted a writ of mandamus?” I said, “No, Your Honor.” “Zero,” he said, “Zero.” The point is that writs of mandamus are rare. A party must prove to the court that he/she has a clear and indisputable right to what is being asked of the court.
Secondly, in my mind, Cape Fear made a disastrous mistake in arguing that it has a clear right for its Medicare appeals to be adjudicated immediately. Think about it…there are 800,000+ Medicare appeals pending before the ALJs. What judge would ever order the administrative court to immediately drop all other 799,250 pended claims (Cape Fear had 750 claims pending) and to adjudicate only Cape Fear’s claims? It is the classic slippery slope…if you do this for Cape Fear, then you need to order the same for the rest of the pended claims.
In this instance, it appears that Cape Fear requested too drastic a measure for a federal judge to order. The claims were doomed from the beginning.
However, I cannot fault Cape Fear for trying since the code is crystal clear in requiring a 90-day turnaround time. The question becomes…what is the proper remedy for a gross disregard, even if unwillful, of the 90-day turnaround period?
This would have taken thinking outside the box.
Medicare providers have some rights. I discuss those rights frequently on this blog. But the population that the courts inevitably want to insulate from “David and Goliath situations” are the recipients. Unlike the perceived, “big, strong, and well-attorneyed” hospital, recipients often find themselves lacking legal representation to defend their statutorily-given right to choose their provider and exercise their right to access to care.
Had Cape Fear approached the same problem from a different perspective and argued violations of law on behalf of the beneficiaries of Cape Fear’s quality health care services, a different result may have occurred.
Another way Cape Fear could have approached the same problem, could have been a request for the Court to Cape Fear’s funds owed for service rendered to be released pending the litigation.
As always, there is more than one way to skin a cat. I humbly suggest that when you have such an important case to bring…BRING IT ALL!!
CMS’ Feeble Attempt to Decrease Medicare Appeal Backlog Will, At Least, Benefit Providers
On August 1, 2015, the Center for Medicare and Medicaid Services (CMS) clarified (limited) the scope of Medicare auditors in a published article entitled, “Limiting the Scope of Review on Redeterminations and Reconsiderations of Certain Claims.” (MLN Matters® Number: SE1521).
The limitations apply to Medicare Audit Contractors (MACs) and Qualified Independent Contractors (QICs). This new instruction will apply to audits conducted on or after August 1, 2015, and will not be applied retroactively. Important to note: this instruction does not apply to prepayment review, only post payment reviews.
MLN Matters® Number: SE1521 was published in response to the overwhelming, increasingly, mushroomed backlog of Medicare appeals at the Administrative Law Judge (ALJ) level. Six years ago, prior to the Affordable Care Act (ACA), the number of Medicare appeals at the ALJ level was sustainable. Six years later, in 2015, the Medicare appeal backlog has skyrocketed to numbers beyond the comprehension of any adversely affected health care provider, i.e., over 547 days for adjudication!
So in order to combat these overwhelming, bottle-necked and “anything but speedy Medicare appeals,” CMS attempted to rectify the situation by setting new limitations (among other measures) as to the scope of authority that MACs and QICs may present on an audit. However, these new limitations remind me of the hole that is in my front yard. Yes, a hole. The title of this story is “Inertia: What is Easy to Keep Going, Is Impossible to Pull Back” or “I love my husband’s intentions, but the result looks like the Medicare backlog.”
My wonderful husband and I purchased a small farm at the beginning of the year. If you have been following my blog over the past year, you will know that we have horses, peacocks, a micro pig, two dogs, and a 10-year-old. It is a whirlwind of fun.
Well, included in our purchase was a very shallow, very mosquito-ridden pond. It was about 4-5 inches deep and I never really thought about it. It was a pond. It was not beautiful, but it was not ugly. It was just there.
My husband tells me one day that he is going to “clean out the pond.”
BEFORE (except he already tore up the grass, so I do not have a true before picture):

Every day, for three months, I come home to a deeper and deeper pond.
“I’m bound to hit a spring,” he would say. Or “Leroy says that there is a lot of water under our ground.” How Leroy came to this conclusion, I do not know. But, slowly, and almost unperceptively, each day the hole grows wider and deeper.
Until, one day, I come home to this:
AFTER:

It would be funny if it were in your yard. (BTW: For scale, check out the horses (one is white, one is brown) in the top left corner.)
“I love my husband’s intentions, but the result looks like the Medicare backlog.”
You cannot undo digging a hole in your front yard that could swallow an elephant..or maybe two or three elephants. Just like you cannot undo a Medicare appeal backlog that could, potentially, fill my hole with its paperwork. You just have to make do, sit on your front porch, and admire the meteor-like hole that resides in your front lawn.
We (He) have (has) high hopes that our hole will become a lake or a swimming hole. In order to help the cause, I spit in it every time I walk by it. In the alternative, we sometimes aim the sprinkler toward the hole and let it run for a few hours. These are examples of our attempts of reconciling our hole into a beautiful swimming hole.
Similarly, when CMS created these MACs and QICs for Medicare audits, at first, it seemed that the MACs and QICs had no limits as to their scopes of authority to audit. Due to these overzealous and, sometimes, overreaching audits, the appeal backlog increased in number, then multiplied. Similar to the construction of my hole, the appeal backlog grew slowly, at first, then exponentially until the backlog is out of hand and uncontrollable. See blog.
One example of the seemingly limitless authority that the MACs and QICs wielded was that the auditors would provide reasons why claims were noncompliant, the defect could be cured, and the MACs and/or QICs would deny the claim for an entirely different reason.
The auditor would, in essence, be moving the goalposts after you kicked the ball. And the appeal backlog continued to swell.
The ability for the auditors to expand the review of claims beyond which was initially reviewed contributed the massive backlog of Medicare appeals at the ALJ level because more providers appeal an audit with which they disagree (common sense). Just like my hole in my front yard, the backlog of appeals grew, then ballooned until the number of Medicare appeals stuck in the backlog could possibly fill my hole. See blog for the Medicare appeal process and appeal deadlines.
According to the most current statistics available, there is a Medicare appeal backlog of approximately 870,000 appeals. The average processing time for appeals decided in fiscal year 2015 is 547.1 days.

Look at the balloon effect of “average processing time by fiscal year.” In 2009, the average processing time was 94.9 days (a little over 3 months). Now it is over 540 days (almost a year and a half)!!
“I love my husband’s intentions, but the result looks like the Medicare backlog.”
In an attempt to clear the backlog, CMS released MLN Matters® Number: SE1521, on August 1, 2015, in which “CMS has instructed MACs and QICs to limit their review to the reason(s) the claim or line item at issue was initially denied.” (emphasis added).
An exception, however, is if claims are denied for insufficient documentation and the provider submits documents, the claim may still be denied for lack of medical necessity if the documents submitted do not support medical necessity.
This new instruction found in MLN Matters No. SE1521 is an attempt by CMS to reconcile the huge backlog of Medicare appeals at the ALJ level. It is a small gesture. Quite frankly, this instruction should be self-evident as it is inherently unfair to providers to move the goalposts during an audit. I liken this gesture to my husband aiming the sprinkler toward the hole.

In other words, in my opinion, this feeble gesture alone, will not solve the problem. But, in the meantime, it will benefit providers who have been suffering from the goalposts being moved during an audit.
Once something is so big…
“I love my husband’s intentions, but the result looks like the Medicare backlog.”
Maybe the backlog will be fixed when my hole has transformed to a swimming hole.
NCTracks: There’s a Hole in My Bucket !!
My mom taught me a song when I was young called, “A Hole in the Bucket.” It is a maddening song about a lazy husband named Henry who begins the song telling his wife Liza that “There’s a hole in the bucket, dear Liza, dear Liza….” To which Liza sings, “Then fix it, dear Henry, dear Henry…”
The song continues with Henry singing excuses and impediments to his ability to fix the hole in the bucket and Liza explaining to Henry how to overcome these excuses. The song goes around and around until, in order to fix the bucket, Henry would have to sharpen an ax on a stone that “is too dry,” and the only way to wet the stone is with the bucket that has a hole. “There’s a hole in the bucket…” And the songs starts anew and can be sung continuously, never-ending.
My husband and daughter audibly groan when I begin such song.
And you can’t blame them! It is discouraging and frustrating when something is caught in a never-ending circle with no end and no conclusion. It is human nature to try to resolve issues; it is also ingrained in Americans’ minds that hard work yields results. When hard work yields nothing but a big, fat goose-egg, it is exacerbating.
Kind of like claims in NCTracks…
When NCTracks went live on July 1, 2013, providers immediately began to complain the claims were being erroneously denied and they were receiving no reimbursements. Folks with whom I spoke with were at their wits-ends, spending hours upon hours trying to discern why claims were being denied and what process they could undertake to fix “the hole in the bucket.”
The problem persisted so long and I was contacted by so many providers that I instigated the NCTracks class action lawsuit, which is still pending on appeal, to the best of my knowledge, at my former firm. Although it was dismissed at the Business Court level, I believe it is on appeal. See blog.
Providers complained that, when they contacted CSC’s Help Desk regarding denied claims, the customer service representatives would have little to no understanding of the claims process and instruct them to re-file the denied claims, which created a perpetual cycle of unadjudicated claims.
“It was infuriating!” One provider explained. “It was as if we were caught in the spin cycle with no hope of stopping. I wanted to yell, ‘I’m dry all ready!!'”
“I was spending 20+ a week on NCTracks billing problems,” another said.
To which, I said, “There’s a hole in the bucket, dear Liza, dear Liza.”
Over two years after the “go live” date, the Department has now (finally) informed providers that there is an informal reconsideration review process for denials from CSC.
The September 2015 Medicaid Bulletin states that:
“This article provides a detailed explanation of the N.C. Division of Medical Assistance (DMA) procedures for Informal Reconsideration Review of adverse claim actions (denials, disallowances and adjustments) made by its fiscal agent, CSC.”
The Bulletin provides a 30 day time period during which a provider can appeal a denied claim:
“Time Limit for Submission of Request
- A provider may request a reconsideration review within 30 calendar days from receipt of final notification of payment, payment denial, disallowances, payment adjustment, notice of program reimbursement and adjustments. If no request is received within the respective 30 calendar day period, DMA’s action will become final.”
(emphasis in original).
You must request reconsideration review within 30 calendar days of the final notification. BUT what exactly is “final notification?” The initial denial? The second denial after re-submitting? The third? Or, what if, your claim is pending…for months…is that a denial? When CSC tells you to re-submit, does the time frame in which to file a reconsideration review start over? Or do you have to appeal every single denial for every single claim, even if the claim is re-submitted and re-denied 10 times?
This new informal appeal process is as clear as mud.
Notice the penalty for NOT appealing within 30 days…”DMA’s action will become final.”
This means that, if you fail to appeal a denial within 30 days, then the claim is denied and you cannot request a reconsideration review. Theoretically, there is a legal argument that, once the “final decision” is rendered, even if it were rendered due to you failing to request a reconsideration review, you would have 60 days to appeal such final decision to the Office of Administrative Hearings (OAH). Although, acting as the Devil’s advocate, there is an argument that your failure to request a reconsideration review and taking the appeal straight to OAH is “failing to exhaust your administrative remedies.” See blog. Which could result in your appeal being dismissed for lack of jurisdiction. This goes to show you the importance of having your attorney involved at the earliest juncture, otherwise you could risk losing appeal rights.
Let’s think about the “time limit for submission of request” in a real-life hypothetical.
You keep receiving denials for dialysis claims for no apparent reason. You received 20 denials on September 4, 2015. You contact a CSC customer service representative on September 8, 2015, four days later, due to Labor Day weekend. The customer service representative instructs you to re-file the claims because you must include the initial date of treatment in order to have the claims processed and paid (which was not required with HP Enterprises’ system). Is this the “final notification?” It does not seem so, since you are allowed to re-submit…
You revise all 20 claims to include the first treatment date on the claim and re-submit them on September 9, 2015. Since you re-submitted prior to the September 10th cutoff, you expect payment by September 16, 2015, 12 days after the initial denial.
You receive your explanation of benefits (EOBs) and 5 claims were adjudicated and paid, while 15 were denied again.
You contact CSC customer service and the representative instructs you to re-submit the 15 claims. The rep does not know why the claims were denied, but she/he suggests that you review the claims and re-submit. After hours of investigative work, you believe that the claims were denied because the NPI number was wrong…or the incorrect address was processed…or…
You miss the September 17th cut-off because you were trying to figure out why these claims were denied. you submit them for payment for the September 29th checkwrite date (25 days after the initial denial).
At this point, if any claims are denied, you wouldn’t know until October 6th, 32 days after the initial denial.
In my scenario, when is the final adjudication?
If the answer is that the final adjudication is at the point that the provider tries all possible revisions to the claims and continues to re-submit the claims until he/she cannot come up with another way to re-submit, then there is never final adjudication. As in, the provider could continue various changes to the billing ad nauseam and re-submit…and re-submit…and re-submit…”There’s a hole in the bucket!”
If the answer is that the final adjudication is the initial denial, then, in my scenario, the provider would be required to appeal every single denial, even for the same claim and every time it is denied.
You can imagine the burden to the provider if my second scenario is correct. You may as well hire a full-time person whose only task is to appeal denied claims.
Regardless, this new “Informal Reconsideration Review” purports to create many more questions than answers.
So may rules are enacted with good intentions, but without the “real life” analysis. How will this actually affect providers?
“There’s a hole in the bucket, dear Liza, dear Liza.”
“Then fix it.”
Another Win for the Good Guys! Gordon & Rees Succeeds in Overturning Yet Another Medicaid Contract Termination!
Getting placed on prepayment review is normally a death sentence for most health care providers. However, our health care team here at Gordon Rees has been successful at overturning the consequences of prepayment review. Special Counsel, Robert Shaw, and team recently won another case for a health care provider, we will call her Provider A. She had been placed on prepayment review for 17 months, informed that her accuracy ratings were all in the single digits, and had her Medicaid contract terminated.
We got her termination overturned!! Provider A is still in business!
(The first thing we did was request the judge to immediately remove her off prepayment review; thereby releasing some funds to her during litigation. The state is only allowed to maintain a provider on prepayment review for 12 months).
Prepayment review is allowed per N.C. Gen. Stat. 108C-7. See my past blogs on my opinion as to prepayment review. “NC Medicaid: CCME’s Comedy of Errors of Prepayment Review” “NC Medicaid and Constitutional Due Process.”
108C-7 states, “a provider may be required to undergo prepayment claims review by the Department. Grounds for being placed on prepayment claims review shall include, but shall not be limited to, receipt by the Department of credible allegations of fraud, identification of aberrant billing practices as a result of investigations or data analysis performed by the Department or other grounds as defined by the Department in rule.”
Being placed on prepayment review results in the immediate withhold of all Medicaid reimbursements pending the Department of Health and Human Services’ (DHHS) contracted entity’s review of all submitted claims and its determination that the claims meet criteria for all rules and regulations.
In Provider A’s situation, the Carolinas Center for Medical Excellence (CCME) conducted her prepayment review. Throughout the prepayment process, CCME found Provider A almost wholly noncompliant. Her monthly accuracy ratings were 1.5%, 7%, and 3%. In order to get off prepayment review, a provider must demonstrate 70% accuracy ratings for 3 consecutive months. Obviously, according to CCME, Provider A was not even close.
We reviewed the same records that CCME reviewed and came to a much different conclusion. Not only did we believe that Provider A met the 70% accuracy ratings for 3 consecutive months, we opined that the records were well over 70% accurate.
Provider A is an in-home care provider agency for adults. Her aides provide personal care services (PCS). Here are a few examples of what CCME claimed were inaccurate:
1. Provider A serves two double amputees. The independent assessments state that the pateint needs help in putting on and taking off shoes. CCME found that there was no indication on the service note that the in-home aide put on or took off the patients’ shoes, so CCME found the dates of service (DOS) noncompliant. But the consumers were double amputees! They did not require shoes!
2. Provider A has a number of consumers who require 6 days of services per week based on the independent assessments. However, many of the consumers do not wish for an in-home aide to come to their homes on days on which their families are visiting. Many patients inform the aides that “if you come on Tuesday, I will not let you in the house.” Therefore, there no service note would be present for Tuesday. CCME found claims inaccurate because the assessment stated services were needed 6 days a week, but the aide only provided services on 5 days. CCME never inquired as to the reason for the discrepancy.
3. CCME found every claim noncompliant because the files did not contain the service authorizations. Provider A had service authorizations for every client and could view the service authorizations on her computer queue. But, because the service authorization was not physically in the file, CCME found noncompliance.
Oh, and here is the best part about #3…CCME was the entity that was authorizing the PCS (providing the service authorizations) and, then, subsequently, finding the claim noncompliant based on no service authorization.
Judge Craig Croom at the Office of Administrative Hearings (OAH) found in our favor that DHHS via CCME terminated Provider A’s Medicaid contract arbitrarily, capriciously, erroneously, exceeded its authority or jurisdiction, and failed to act as accordingly to the law. He ruled that DHHS’ placement of Provider A on prepayment review was random
Because of Judge Croom’s Order, Provider A remains in business. Plus, she can retroactively bill all the unpaid claims over the course of the last year.
Great job, Robert!!! Congratulations, Provider A!!!


